 IJCP Editorial Team
IJCP Editorial Team
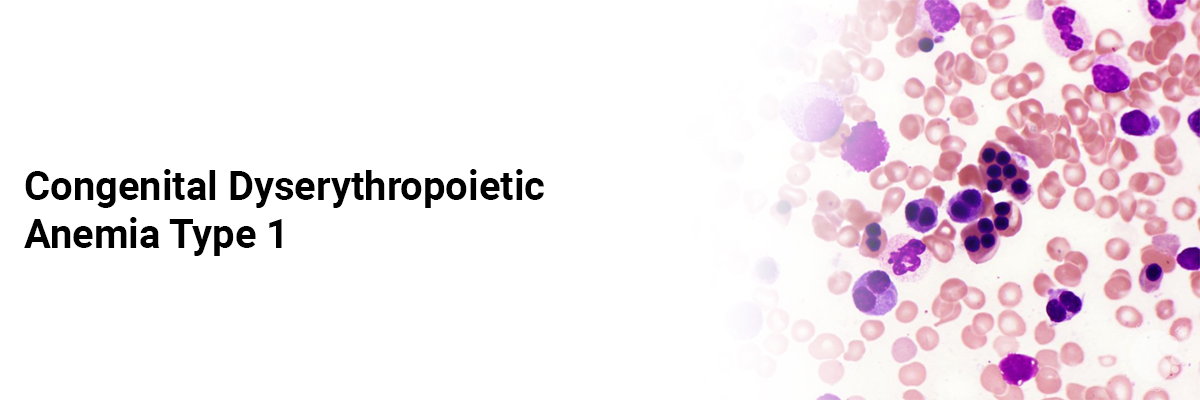
Congenital Dyserythropoietic Anemia Type 1
The
parents of a six-month-old male infant complained that the child had developed
a fever over the last three days after an episode of paleness, which persisted
for the last 20 days.
The
baby was the firstborn from his non-consanguineous parents. There was no
history of recent bleeding episodes or prior blood transfusions. The child was
exclusively breastfed and showed regular developmental progress.
Physical
examination revealed a body weight of 6 kg, length - 64 cm, and head
circumference - 42 cm. His vitals showed – a heart rate of 140 beats per
minute, respiratory rate of 42 breaths per minute, facial puffiness, peripheral
edema, and evident pallor. Abdominal examination revealed non-tender, soft
hepatomegaly with a liver span of 7 cm and without splenomegaly. Other systemic
examinations appeared normal.
Laboratory
investigations showed:
- Hemoglobin level - 2.8
g/dl
- Red blood cell count
(RBC) - 0.76 million cells/microliter
- White blood cell (WBC)
count - 16,700 cells/microliter
- Platelet count - 115,000
cells/microliter
- Mean corpuscular volume
(MCV) - 94 femtoliters
A
peripheral blood smear indicated anisopoikilocytosis, primarily with normocytic
normochromic RBCs, displaying macrocytosis. Liver function tests showed:
- Serum total bilirubin -
2.70 mg/dl
- Unconjugated bilirubin -
1.6 mg/dl
- AST - 60 U/L
- ALT - 17 U/L
- Alkaline phosphatase - 83
U/L
Serum
electrolytes and creatinine levels were within the normal range. Serum ferritin
levels were elevated at 975 ng/dl, and the reticulocyte count was 12.5, with a
corrected reticulocyte count of 2.4%. Vitamin B12 deficiency was excluded.
High-performance liquid chromatography testing for hemoglobinopathies returned
negative results. Abdominal ultrasonography did not reveal gallstones.
Subsequent
bone marrow examination showed hypercellularity with erythroid hyperplasia.
Erythropoiesis displayed megaloblastic characteristics, such as nuclear
budding, micronuclei, multinuclearity, and multipolar mitosis. Erythroblasts
exhibited chromatin bridges, with occasional red blood cells showing basophilic
stippling.
The
findings led to the diagnosis of congenital dyserythropoietic anemia. The
acidified serum lysis test (HEMPAS) yielded negative results, and genetic
studies were unavailable. The diagnosis of CDA type 1 was made based on the
early age of presentation, the presence of megaloblastic cells on the
peripheral smear, internuclear chromatin bridges between erythroblasts on bone
marrow examination, and the negative HEMPAS test.
The
infant received packed red cell transfusions and symptomatic treatment.
Following discharge, the child continued to be monitored and required further
transfusions during follow-up.
CDA 1 should be considered in cases of refractory anemia, hepatosplenomegaly, erythroid hyperplasia, and features of dyserythropoiesis observed in marrow examinations. Hyperbilirubinemia and unexplained iron overload should also raise suspicion of CDAs. The diagnosis of CDA 1 can be based on typical characteristics observed in peripheral blood smears and bone marrow examinations.
Source: Chandel AS,
Itihas A, Jategaonkar S, Jain M, Paediatrics MS. NIJP. 2019 Oct;8:4.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs



Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article