 IJCP Editorial Team
IJCP Editorial Team
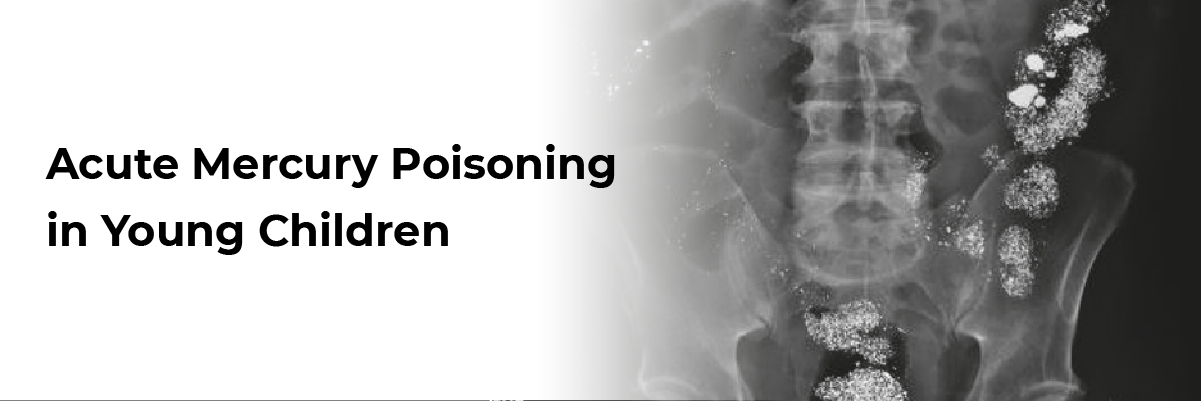
Acute Mercury Poisoning in Young Children
A report describes a case of a 21-month-old boy who presented with alleged accidental consumption of 120 mg of inorganic mercury three days back. He experienced mild cough and coryza, vomiting, and pain abdomen. Lab reported his blood mercury level to be 16.5 μg/L.
The physicians administered Oral Dimer- captosuccinic acid (DMSA) (10 mg/kg/dose TDS for 5 d followed by 10 mg/kg/dose BD for the next 2 wk). His urine mercury levels before and 3 d after starting DMSA were 16 μg/L and 60 μg/L, respectively. After 7 d of therapy, his blood mercury levels decreased to 10 μg/L, and he received a discharge in stable condition.
Centers for Disease Control and Prevention (CDC) defines >10 μg/L as the toxic levels of mercury in blood. Although very young children are more sensitive to mercury than adults, it remains unclear when to start the antidote therapy in cases with mild symptoms but marginally higher blood mercury levels. Moreover, blood mercury levels increase rapidly after exposure.
Different laboratory cut-offs also influence the antidote treatment decision (normal blood mercury range: 0.2–1.3 μg/L). One popular reference range is 0.6–59 μg/L. Hence, starting an antidote may be a tough decision. The discussed case received an antidote for the following reasons: blood mercury levels on day 3 were in the toxic range; acute mercury exposure was unrelated to food, the younger age of the patient, and mild symptoms.
Acute Mercury Poisoning in Young Children: When to Treat? Indian Journal of Pediatrics. 2023.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs



Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article