

 Dr. Ambika Kapoor
Dr. Ambika Kapoor
Know What causes Acne? Symptoms and Treatment
Type | Symptoms | Causes | Diagnosis | Treatment
Acne vulgaris, also known as acne, is a long-term skin disease in which dead skin cells and oil from the skin clog hair follicles.
Blackheads or whiteheads, pimples, dry skin, and scarring are all common symptoms of the disease. (1) (2) (11)
It mainly affects skin with a high number of oil glands, which includes the face, upper chest, and back. Anxiety, low self-esteem, and, in severe cases, depression may result from the presence of acne on one’s skin, especially the face. (3) (4)
Acne affects approximately 70 crore people worldwide each year, making it the eighth most prevalent disease. (9)
Acne is a widespread adolescent ailment that affects an estimated 80–90% of adolescents in the Western world.
Acne is less common in some rural communities than in urban areas. Before and after puberty, both children and adults can be affected. While acne becomes less frequent as people get older, it still affects nearly half of those who have it in their twenties and thirties, and a smaller number of people in their forties. (2)
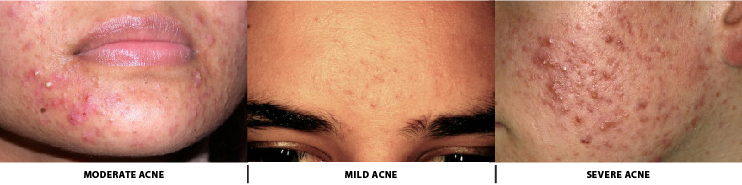
Types of Acne Based on Severity
To determine an effective treatment regimen, the severity of acne vulgaris may be categorized as mild, moderate, or serious. Acne intensity is not graded on a widely agreed scale.
Mild acne is described by the appearance of clogged skin follicles (comedones) on the face with occasional inflammatory lesions. (12) (13)
When a higher number of inflammatory papules and pustules appear on the face compared to mild cases of acne that appear on the trunk of the body, it is said to be moderate intensity acne.
When nodules (painful 'bumps' under the skin) are the primary facial lesions and the trunk is heavily involved, severe acne is said to be present. (12) (13)
Acne inversa and acne rosacea are alternative names for the skin conditions hidradenitis suppurativa (HS) and rosacea, respectively.
Signs & Symptoms of Acne
Acne is characterized by increased oily sebum secretion by the skin, as well as microcomedones, comedones, papules, nodules (large papules), pustules, and scarring. Acne appears differently depending on the color of the skin. It could lead to psychological and social issues. (13)
1.Scars
Inflammation of the dermis causes acne scarring. The scar is caused by abnormal healing and dermal inflammation. Scarring is most common in extreme acne, but it can happen in any type of acne vulgaris.
Acne scars are categorized according to whether an irregular healing reaction to dermal inflammation results in excessive collagen deposition or loss at the acne lesion site. (14) (15)
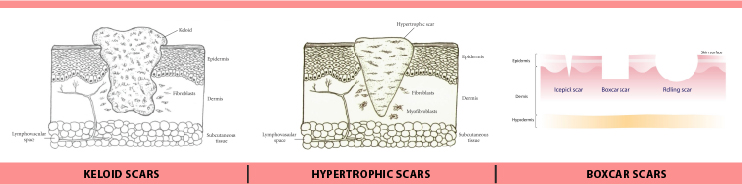
The most common form of acne scar is atrophic acne scars, which have lost collagen as a result of the healing response (accounting for approximately 75 percent of all acne scars). Atrophic acne scars are divided into three types: ice-pick scars, boxcar scars, and rolling scars.
Boxcar scars are indented scars that are round or ovoid in shape and have sharp borders. They range in size from 1.5–4 mm across. Ice-pick scars are deep scars that reach into the dermis and are narrow (less than 2 mm across). Rolling scars are larger (4–5 mm across) than ice-pick and boxcar scars and have a wave-like pattern of depth in the skin. (14) (15)
Hypertrophic scars are rare and are defined by an increase in collagen content following an irregular healing response. They are firm and lifted from the skin, according to.
Keloid scars may form scar tissue outside of the original wound margins, while hypertrophic scars stay within the wound's original margins. (14) (15)
Acne scars that develop into keloid scars are more common in men and people with darker skin, and they typically appear on the trunk of the body. (14) (15)
2.Pigmentation
When an inflamed nodular acne lesion heals, the skin in that area often darkens, a condition known as postinflammatory hyperpigmentation (PIH). The inflammation causes melanocytes (specialized pigment-producing skin cells) to produce more melanin pigment, resulting in the darkened appearance of the skin. People with darker skin are more likely to develop PIH. (16)
The word "pigmented scar" is often used to describe PIH, but it is misleading because it implies that the color change is permanent. PIH is also preventable by preventing aggravation of the nodule, and it fades with time. If the deeper layers of the skin are affected, untreated PIH can last for months, years, or even be permanent.
Even a small amount of skin exposure to ultraviolet rays from the sun can cause hyperpigmentation. Using a sunscreen with SPF-15 or higher on a daily basis will help to reduce this risk. (16)
Causes of Acne
Other than genetics, no definitive risk factors for the development of acne have been reported. Hormones, pathogens, diet, and stress are all potential secondary contributors. Studies on the effect of smoking on the occurrence and intensity of acne have shown mixed results. Acne is not linked to sunlight or cleanliness. (2)
1.Genetics
Acne tends to be heavily inherited; genetics accounts for 81% of population variation. Studies on acne in affected twins and first-degree relatives show that the condition is heavily inherited.
Since acne may not adopt a classic Mendelian inheritance pattern, vulnerability to the disease is possibly attributable to the impact of multiple genes. (2) (12)
Among the gene candidates are variants of the tumor necrosis factor-alpha (TNF-alpha), interleukin-1 alpha (IL-1 alpha), and CYP1A1 genes, among others.
A mutation in the gene for TNF called the 308 G/A single nucleotide polymorphism has been linked to an increased risk of acne. Acne can be a symptom of rare genetic conditions like Apert's syndrome. XYY syndrome can be linked to severe acne. (12)
2.Hormones
Hormonal activity, such as that seen during menstrual cycles and puberty, can play a role in acne development.
The skin follicle glands develop larger and produce more oily sebum as a result of a rise in sex hormones called androgens during puberty.
Acne is related to the androgen hormones testosterone, dihydrotestosterone (DHT), and dehydroepiandrosterone (DHEA). (17)
Acne is also linked to high levels of growth hormone (GH) and insulin-like growth factor 1 (IGF-1). (42nd) Acne does not develop in people who have complete androgen insensitivity syndrome (CAIS) or Laron syndrome, indicating that both androgens and IGF-1 are needed for acne to develop (insensitivity to GH, resulting in very low IGF-1 levels).
Acne may be caused by medical conditions that induce a high-androgen state, such as polycystic ovary syndrome, congenital adrenal hyperplasia, and androgen-secreting tumors. (17) (18)
Pregnancy can raise androgen levels, which leads to an increase in oily sebum production. Acne may be a side effect of testosterone replacement therapy (TRT) or anabolic steroid use. Anabolic steroids are commonly used in over-the-counter bodybuilding and dietary supplements.
3.Infections
Cutibacterium acnes (formerly Propionibacterium acnes) is an anaerobic bacterial species that plays a role in the production of acne, but its exact role is unknown. C.
acnes has sub-strains that are associated with normal skin and others that are associated with moderate to severe inflammatory acne. (2) (19)
Biofilms are formed when S. epidermidis and C. acnes coexist, blocking hair follicles and pores and creating an anaerobic environment, promoting their growth beneath the skin.
The growth of C. acnes leads to the formation of a biofilm matrix, making acne treatment even more difficult. (19)
4.Dietary Habits
Diets with a high glycemic load have been shown to have varying degrees of impact on acne severity. A lower-glycemic-load diet has been shown to be efficient in reducing acne in several randomized controlled trials and nonrandomized studies. (7)
Only a few studies have looked into the connection between obesity and acne. When consumed in excess of the recommended daily intake, vitamin B12 can cause acne-like skin outbreaks (acneiform eruptions) or exacerbate existing acne. (19)
A meta-study published in 2021 discovered high-glycemic foods, dairy products, fat foods, and chocolate are acne-promoting factors, while fatty acids, fruit, and vegetable intake are acne-protective. (2)
5.Stress
There are only a few high-quality studies that show stress induces or aggravates acne. Despite being controversial, some evidence suggests that in some circumstances, such as hormonal changes seen in premenstrual syndrome, elevated acne incidence is linked to high stress levels.
6.Other Causes
Mechanical obstruction of skin follicles with helmets or chin straps may exacerbate pre-existing acne.
Pre-existing acne may be aggravated by a number of drugs. Lithium, hydantoin, isoniazid, glucocorticoids, iodides, bromides, and testosterone are examples of such drugs.
Clinical Diagnosis of Acne
Acne vulgaris is diagnosed based on the clinical assessment of a medical practitioner. A comprehensive medical history regarding a family history of acne, a study of drugs taken, and signs or symptoms of increased development of androgen hormones, cortisol, and growth hormone should all be taken into account when evaluating an individual with suspected acne. (1)
Acne must have comedones (blackheads and whiteheads) to be diagnosed. The absence of comedones is suggestive of skin conditions other than acne.
Treatment of Acne
Acne can be treated in a variety of ways. Reduced inflammation, hormonal manipulation, killing C. acnes, and normalizing skin cell shedding and sebum production in the pore to prevent blockage are just a few of the ways acne treatments work.
Topical retinoids, benzoyl peroxide, and topical or oral antibiotics are all recommended as first-line treatments for acne vulgaris. Owing to their high cost and lack of evidence, procedures like light therapy and laser therapy are not first-line therapies and are typically used as a supplement.
1.Skin Care Regimen
In general, people with acne should not wash their infected skin more than twice a day. Using a fragrance-free moisturizer on sensitive and acne-prone skin will help to minimize irritation. (20)
Acne medication-induced skin irritation typically peaks two weeks after first use and improves with continued use. Dermatologists advise that you use cosmetics that are non-comedogenic, oil-free, and won't clog your pores. (20)
2.Diet
Medical diet therapy appears to be effective in reducing the severity and prevalence of dermatologic disorders, including acne. Diets with a high glycemic index have been linked to acne, according to research. (19)
A diet low in simple sugars is also recommended by dermatologists as a way to improve acne. As of 2014, the evidence supporting the use of milk restriction for this purpose was inadequate.
3.Medications
A) Benzoyl peroxide
Because of its efficacy and low side effects, benzoyl peroxide (BPO) is a first-line treatment for mild to moderate acne (mainly skin irritation). Benzoyl peroxide kills C. acnes in the skin follicle by oxidizing its proteins and producing oxygen free radicals and benzoic acid. The bacterium's metabolism and ability to produce proteins are likely to be affected by these free radicals. (21)
B) Retinoids
Retinoids are anti-inflammatory drugs that help to normalize the follicle cell life cycle and lower sebum development. They have a similar structure to vitamin A. The cell life cycle in the follicle lining seems to be influenced by retinoids. This keeps skin cells from accumulating inside the hair follicle and causing a blockage. (22)
They're a go-to acne treatment, particularly for people with dark-colored skin. Retinoids are known to lead to faster improvement of postinflammatory hyperpigmentation. (1) (22)
Adapalene, retinol, tazarotene, trifarotene, and tretinoin are all topical retinoids used for acne treatment. Isotretinoin is an oral retinoid that is very effective for severe nodular acne, and moderate acne that is stubborn to other treatments. (22)
C) Antibiotics
Antibiotics may be applied to the skin or taken orally to treat acne. They kill C. acnes while also reducing inflammation. Due to prevalence of antimicrobial resistance amongst bacteria, Antibiotics are best used in conjunction with other treatments rather than on their own by dermatologists. (93)
Clindamycin, erythromycin, metronidazole, sulfacetamide, and tetracyclines are some of the most commonly used antibiotics, whether added to the skin or taken orally (e.g., doxycycline or minocycline). The antibiotic dapsone is effective against inflammatory acne when applied to the skin. (93)
D) Hormonal Agents
Combination birth control pills can help women with acne. Estrogen and progestin are both present in these medications. They function by reducing androgen hormone output by the ovaries, as well as the free and thus biologically active fractions of androgens, resulting in reduced sebum production on the skin and, as a result, a reduction in acne intensity. (24)
Antiandrogens like cyproterone acetate and spironolactone can effectively treat acne, especially in women who show signs of excessive androgen production like increased hairiness, sebum production on the skin, or hair loss on the scalp. (10)
Flutamide, a pure androgen receptor antagonist, is effective in treating female acne. Also at low levels, it tends to reduce acne symptoms by 80 to 90%, with some studies showing full acne clearance. (25)
Antiandrogens may not be used to treat acne in pregnant or lactating women since they can cause birth defects such as hypospadias and feminization of male babies. When taking an antiandrogen, women who are sexually active and who may or may become pregnant should use an appropriate form of contraception to avoid pregnancy. (26) (27)
E) Azelaic acid
When applied topically at a 20% concentration, azelaic acid is useful for mild to moderate acne. Because of its ability to minimize skin cell aggregation in the follicle as well as its antibacterial and anti-inflammatory effects, azelaic acid is an important acne remedy. (1) (28)
Because of its ability to inhibit melanin synthesis, it has a slight skin-lightening effect. As a result, it is useful in treating individuals with acne who are also affected by post-inflammatory hyperpigmentation. (1) (28)
F) Salicylic acid
Salicylic acid is a keratolytic beta-hydroxy acid that can be applied topically to avoid bacteria from reproducing. Salicylic acid clears clogged skin pores and encourages epithelial skin cell shedding. While darkening of the skin can occur in people with darker skin types, the most common side effect of topical application is dry skin. (1) (29)
G) Other Medications
Alternative medical treatments include nicotinamide (Vitamin B3) topical and oral preparations. Because of its anti-inflammatory properties, ability to inhibit sebum development, and wound healing properties, nicotinamide is said to help with acne. (30)
Zinc formulations, both topical and oral, are recommended as acne remedies. Zinc's anti-inflammatory and anti-sebum properties, as well as its ability to inhibit C. acnes growth, are thought to be mechanisms for treating acne. (31)
Because of their anti-inflammatory properties and ability to suppress sebum development, antihistamines can help people who are already taking isotretinoin. (32)
When applied topically, hydroquinone lightens the skin by inhibiting tyrosinase, the enzyme that converts the amino acid tyrosine to the skin pigment melanin. It's used to treat acne-related post-inflammatory hyperpigmentation. (33)
4. Alternative Remedies
Topical application of tea tree oil or bee venom can reduce the total number of skin lesions in acne sufferers, according to low-quality evidence. Tea tree oil tends to be on par with benzoyl peroxide or salicylic acid in terms of effectiveness, although it is linked to allergic contact dermatitis. Some plant-derived remedies, such as basil oil and seaweed, have shown to be effective against acne. (34)
There isn't enough evidence to back up the use of acupuncture, herbal medicine, or cupping therapy to treat acne.
Cosmeceuticals are a type of over-the-counter medication that comes in a variety of types. Acne may be disguised with some forms of makeup. A water-based product is also favored by those with oily skin.
The Social Impact of Acne
Acne has a significant financial and social cost. Acne vulgaris accounts for more than 5 million doctor visits in the United States per year, costing over US$2.5 billion in direct costs. (35) Acne's causative and aggravating factors are often misunderstood, and people often blame acne sufferers for their disease. The victim's self-esteem may be severely affected as a result of such blame.
Acne vulgaris and its resultant scars are associated with significant social and academic difficulties that can last into adulthood. Therefore, it is imperative for society to educate itself about this condition and do away with the stereotypes associated with it.
References:
1. Vary JC (November 2015). "Selected Disorders of Skin Appendages--Acne, Alopecia, Hyperhidrosis". The Medical Clinics of North America (Review). 99 (6): 1195–211. doi:10.1016/j.mcna.2015.07.003. PMID 26476248.
2. Bhate K, Williams HC (March 2013). "Epidemiology of acne vulgaris". The British Journal of Dermatology (Review). 168 (3): 474–85. doi:10.1111/bjd.12149. PMID 23210645. S2CID 24002879.
3. Barnes LE, Levender MM, Fleischer AB, Feldman SR (April 2012). "Quality of life measures for acne patients". Dermatologic Clinics (Review). 30 (2): 293–300, ix. doi:10.1016/j.det.2011.11.001. PMID 22284143.
4. Goodman G (July 2006). "Acne and acne scarring - the case for active and early intervention". Australian Family Physician (Review). 35 (7): 503–4. PMID 16820822. Archived from the original on 21 April 2013.
5. James WD (April 2005). "Clinical practice. Acne". The New England Journal of Medicine (Review). 352 (14): 1463–72. doi:10.1056/NEJMcp033487. PMID 15814882.
6. Kahan S (2008). In a Page: Medicine. Lippincott Williams & Wilkins. p. 412. ISBN 9780781770354. Archived from the original on 6 September 2017.
7. Mahmood SN, Bowe WP (April 2014). "[Diet and acne update: carbohydrates emerge as the main culprit]". Journal of Drugs in Dermatology (Review). 13 (4): 428–35. PMID 24719062.
8. Titus S, Hodge J (October 2012). "Diagnosis and treatment of acne". American Family Physician (Review). 86 (8): 734–40. PMID 23062156. GBD 2015 Disease Injury Incidence Prevalence Collaborators (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
9. Aslam I, Fleischer A, Feldman S (March 2015). "Emerging drugs for the treatment of acne". Expert Opinion on Emerging Drugs(Review). 20 (1): 91–101. doi:10.1517/14728214.2015.990373. PMID 25474485. S2CID 12685388.
10. Tuchayi SM, Makrantonaki E, Ganceviciene R, Dessinioti C, Feldman SR, Zouboulis CC (September 2015). "Acne vulgaris". Nature Reviews. Disease Primers. 1: 15033. doi:10.1038/nrdp.2015.33. PMID 27227877. S2CID 44167421
11. Tuchayi SM, Makrantonaki E, Ganceviciene R, Dessinioti C, Feldman SR, Zouboulis CC (September 2015). "Acne vulgaris". Nature Reviews. Disease Primers. 1: 15033. doi:10.1038/nrdp.2015.33. PMID 27227877. S2CID 44167421.
12. Dawson AL, Dellavalle RP (May 2013). "Acne vulgaris". BMJ (Review). 346 (5): 30–33. doi:10.1136/bmj.f2634. JSTOR 23494950. PMID 23657180. S2CID 5331094.
13. Zaenglein AL, Graber EM, Thiboutot DM (2012). "Chapter 80 Acne Vulgaris and Acneiform Eruptions". In Goldsmith, Lowell A., Katz, Stephen I., Gilchrest, Barbara A., Paller, Amy S., Lefell, David J., Wolff, Klaus (eds.). Fitzpatrick's Dermatology in General Medicine (8th ed.). New York: McGraw-Hill. pp. 897–917. ISBN 978-0-07-171755-7.
14. Fife D (April 2016). "Evaluation of Acne Scars: How to Assess Them and What to Tell the Patient". Dermatologic Clinics (Review). 34 (2): 207–13. doi:10.1016/j.det.2015.11.009. PMID 27015781.
15. Levy LL, Zeichner JA (October 2012). "Management of acne scarring, part II: a comparative review of non-laser-based, minimally invasive approaches". American Journal of Clinical Dermatology (Review). 13 (5): 331–40. doi:10.2165/11631410-000000000-00000. PMID 22849351. S2CID 41448330.
16. Chandra M, Levitt J, Pensabene CA (May 2012). "Hydroquinone therapy for post-inflammatory hyperpigmentation secondary to acne: not just prescribable by dermatologists". Acta Dermato-Venereologica (Review). 92 (3): 232–5. doi:10.2340/00015555-1225. PMID 22002814.
17. Das S, Reynolds RV (December 2014). "Recent advances in acne pathogenesis: implications for therapy". American Journal of Clinical Dermatology (Review). 15 (6): 479–88. doi:10.1007/s40257-014-0099-z. PMID 25388823. S2CID 28243535.
18. Housman E, Reynolds RV (November 2014). "Polycystic ovary syndrome: a review for dermatologists: Part I. Diagnosis and manifestations". Journal of the American Academy of Dermatology (Review). 71 (5): 847.e1–847.e10, quiz 857–8. doi:10.1016/j.jaad.2014.05.007. PMID 25437977.
19. Bhate K, Williams HC (April 2014). "What's new in acne? An analysis of systematic reviews published in 2011-2012". Clinical and Experimental Dermatology (Review). 39 (3): 273–7, quiz 277–8. doi:10.1111/ced.12270. PMID 24635060. S2CID 29010884.
20. Zaenglein AL (October 2018). "Acne Vulgaris". The New England Journal of Medicine (Review). 379 (14): 1343–1352. doi:10.1056/NEJMcp1702493. PMID 30281982. S2CID 52914179.
21. Gamble R, Dunn J, Dawson A, Petersen B, McLaughlin L, Small A, et al. (June 2012). "Topical antimicrobial treatment of acne vulgaris: an evidence-based review". American Journal of Clinical Dermatology (Review). 13 (3): 141–52. doi:10.2165/11597880-000000000-00000. PMID 22268388. S2CID 5838346.
22. Riahi RR, Bush AE, Cohen PR (June 2016). "Topical Retinoids: Therapeutic Mechanisms in the Treatment of Photodamaged Skin". American Journal of Clinical Dermatology (Review). 17 (3): 265–76. doi:10.1007/s40257-016-0185-5. PMID 26969582. S2CID 12663356.
23. Barbieri JS, Spaccarelli N, Margolis DJ, James WD (February 2019). "Approaches to limit systemic antibiotic use in acne: Systemic alternatives, emerging topical therapies, dietary modification, and laser and light-based treatments". Journal of the American Academy of Dermatology (Review). 80 (2): 538–549. doi:10.1016/j.jaad.2018.09.055. PMC 6333507. PMID 30296534.
24. Kamangar F, Shinkai K (October 2012). "Acne in the adult female patient: a practical approach". International Journal of Dermatology. 51 (10): 1162–74. doi:10.1111/j.1365-4632.2012.05519.x. PMID 22994662. S2CID 5777817.
25. Bettoli V, Zauli S, Virgili A (July 2015). "Is hormonal treatment still an option in acne today?". The British Journal of Dermatology. 172 Suppl 1: 37–46. doi:10.1111/bjd.13681. PMID 25627824. S2CID 35615492.
26. Azarchi S, Bienenfeld A, Lo Sicco K, Marchbein S, Shapiro J, Nagler AR (June 2019). "Androgens in women: Hormone-modulating therapies for skin disease". Journal of the American Academy of Dermatology. 80 (6): 1509–1521. doi:10.1016/j.jaad.2018.08.061. PMID 30312645.
27. Kong YL, Tey HL (June 2013). "Treatment of acne vulgaris during pregnancy and lactation". Drugs (Review). 73 (8): 779–87. doi:10.1007/s40265-013-0060-0. PMID 23657872. S2CID 45531743.
28. Sieber MA, Hegel JK (November 2013). "Azelaic acid: Properties and mode of action". Skin Pharmacology and Physiology (Review). 27 Suppl 1 (Supplement 1): 9–17. doi:10.1159/000354888. PMID 24280644. S2CID 8848543.
29. Madan RK, Levitt J (April 2014). "A review of toxicity from topical salicylic acid preparations". Journal of the American Academy of Dermatology (Review). 70 (4): 788–792. doi:10.1016/j.jaad.2013.12.005. PMID 24472429.
30. Rolfe HM (December 2014). "A review of nicotinamide: treatment of skin diseases and potential side effects". Journal of Cosmetic Dermatology (Review). 13 (4): 324–8. doi:10.1111/jocd.12119. PMID 25399625. S2CID 28160151.
31. Brandt S (May 2013). "The clinical effects of zinc as a topical or oral agent on the clinical response and pathophysiologic mechanisms of acne: a systematic review of the literature". Journal of Drugs in Dermatology (Review). 12 (5): 542–5. PMID 23652948.
32. Layton AM (April 2016). "Top Ten List of Clinical Pearls in the Treatment of Acne Vulgaris". Dermatologic Clinics (Review). 34 (2): 147–57. doi:10.1016/j.det.2015.11.008. PMID 27015774.
33. Chandra M, Levitt J, Pensabene CA (May 2012). "Hydroquinone therapy for post-inflammatory hyperpigmentation secondary to acne: not just prescribable by dermatologists". Acta Dermato-Venereologica (Review). 92 (3): 232–5. doi:10.2340/00015555-1225. PMID 22002814.
34. Cao H, Yang G, Wang Y, Liu JP, Smith CA, Luo H, Liu Y (January 2015). "Complementary therapies for acne vulgaris". The Cochrane Database of Systematic Reviews (Systematic Review & Meta-Analysis). 1: CD009436. doi:10.1002/14651858.CD009436.pub2. PMC 4486007. PMID 25597924.
35. Knutsen-Larson S, Dawson AL, Dunnick CA, Dellavalle RP (January 2012). "Acne vulgaris: pathogenesis, treatment, and needs assessment". Dermatologic Clinics (Review). 30 (1): 99–106, viii–ix. doi:10.1016/j.det.2011.09.001. PMID 2211787
More FAQs by Dr. Ambika Kapoor



Recent FAQs





Related FAQs



.jpg)


Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article