 IJCP Editorial Team
IJCP Editorial Team
Pediatric Supraglottic Hemangioma Causing Airway Obstruction: A Case Report
Supraglottic hemangiomas are rare vascular malformations of the larynx, particularly in children. They may cause life-threatening airway obstruction if not diagnosed and managed promptly. We report a case of a large supraglottic hemangioma in a young child, presenting with progressive respiratory distress and stridor, successfully managed with endoscopic excision.
Keywords: Supraglottic hemangioma, pediatric airway, vascular malformation, laryngeal obstruction, endoscopic excision
Introduction
Infantile hemangiomas are the most common benign vascular tumors of infancy, typically involving the skin and subcutaneous tissues. Laryngeal involvement is uncommon, with supraglottic localization accounting for a small subset of airway lesions. The reported incidence of airway hemangiomas is approximately 1 in 100,000 live births, with the subglottic region being the most frequently affected site. Early diagnosis is critical because rapid proliferation during infancy can result in severe airway obstruction and respiratory compromise.
Case Presentation
A 2-year-old male presented with a 3-month history of progressive inspiratory stridor, noisy breathing, and intermittent choking episodes. There was no history of cyanosis, hoarseness, or previous airway instrumentation. On examination, the child exhibited mild respiratory distress with inspiratory stridor and suprasternal retraction.
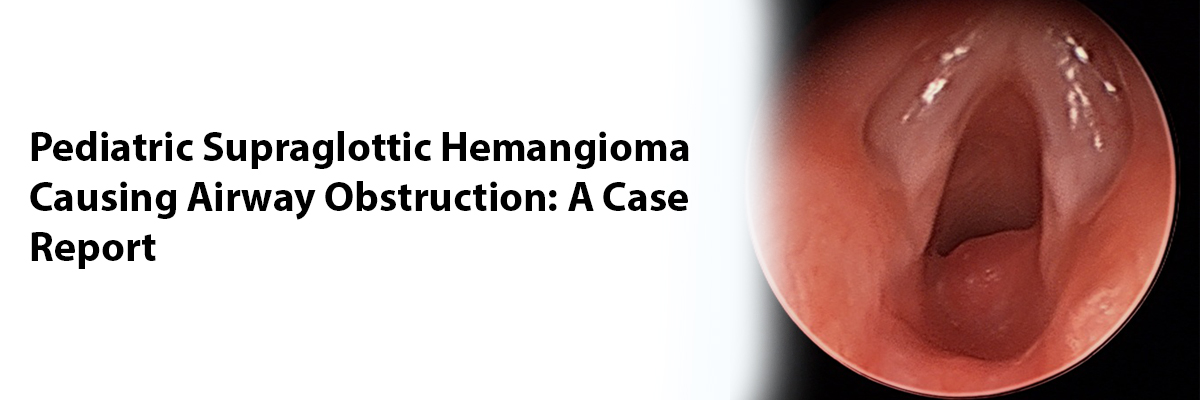
Flexible fiberoptic laryngoscopy revealed a large, smooth, bluish, compressible mass arising from the epiglottis and aryepiglottic folds, partially occluding the supraglottic airway. Contrast-enhanced CT of the neck showed a well-circumscribed, intensely enhancing lesion measuring 2.5 × 2.0 cm in the supraglottic region, suggestive of a vascular tumor.
The child underwent direct laryngoscopy and endoscopic excision under general anesthesia. Intraoperatively, a large hemangiomatous mass involving the epiglottis and aryepiglottic folds was identified. The lesion was excised using cold instruments and laser cautery with minimal bleeding. The airway was secured throughout the procedure.
Histopathology confirmed a capillary hemangioma composed of closely packed capillary-sized vessels lined by flattened endothelium within a fibrous stroma. The postoperative recovery was uneventful, and the child was extubated on the second postoperative day. Follow-up laryngoscopy at 6 months demonstrated complete healing and no evidence of recurrence.
Discussion
Laryngeal hemangiomas are rare and most often present within the first year of life. The supraglottic variant, though less common than subglottic hemangioma, can cause significant airway obstruction. The classic clinical triad includes stridor, feeding difficulties, and voice changes.
Diagnosis is primarily established through flexible laryngoscopy and imaging—typically CT or MRI—to delineate the extent and vascular nature of the lesion. MRI is superior for soft-tissue characterization, but CT with contrast may be more accessible in resource-limited settings.
Management depends on the size, site, and severity of symptoms. Small, asymptomatic lesions may be observed, while symptomatic or rapidly enlarging lesions require intervention. Systemic propranolol has become the first-line therapy for infantile hemangiomas, inducing regression via vasoconstriction, decreased angiogenic signaling, and apoptosis of endothelial cells. However, in cases with large, obstructive, or non-responsive lesions—as in our case—surgical excision or laser ablation remains the treatment of choice.
Advances in endoscopic techniques, including the use of CO₂ or KTP lasers, have significantly improved outcomes by allowing precise removal with minimal bleeding and tissue damage. Long-term follow-up is essential to monitor for recurrence or residual airway compromise.
Conclusion
Supraglottic hemangiomas, though rare, should be considered in the differential diagnosis of persistent stridor in children. Early airway assessment and individualized treatment planning are essential. Endoscopic excision provides an effective and safe therapeutic option for large, symptomatic lesions, ensuring complete relief of obstruction and favorable long-term outcomes.
References
1. Perkins JA, Duke W, Chen EY, Manning SC. Propranolol therapy for airway hemangiomas: a paradigm shift. Laryngoscope. 2009;119(10):2059-2066.
2. Wyatt ME, Hartley BE, Roebuck DJ, Evans JN, Bailey CM. Upper airway haemangiomas: diagnosis and management. Clin Otolaryngol Allied Sci. 2003;28(5):391-399.
3. Dedo HH, Sooy CD. Infantile hemangioma of the larynx: a 20-year experience with laser and steroid therapy. Laryngoscope. 1984;94(6):676-682.
4. Buckmiller LM. Update on hemangiomas and vascular malformations. Curr Opin Otolaryngol Head Neck Surg. 2004;12(6):476-487.
5. Chang LC, Haggstrom AN, Drolet BA, et al. Growth characteristics of infantile hemangiomas: implications for management. Pediatrics. 2008;122(2):360-367.
6. Wang Z, Zhang L, Han W, et al. Management of infantile airway hemangioma: a single-center experience. Int J Pediatr Otorhinolaryngol. 2020;136:110167.
7. Leboulanger N, Fayoux P, Teissier N, et al. Propranolol for severe infantile laryngeal hemangiomas: preliminary report. Pediatrics. 2010;126(2):e418-e421.
8. Bitar MA, Moukarbel RV, Zalzal GH. Management of congenital subglottic hemangioma: trends and success over the past 17 years. Otolaryngol Head Neck Surg. 2005;132(2):226-231.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs



Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article