 IJCP Editorial Team
IJCP Editorial Team
Managing Pediatric intratesticular abscess with a testicular sparing approach
A report describes a case of a 6-year-old boy with no significant past medical or surgical history who presented with left lower abdominal pain for two days. He refused urinary symptoms.
On physical examination, the patient was afebrile and displayed a soft and non-tender abdomen with localized tenderness over the superior and lateral aspect of the left testicle. His scrotum was otherwise normal. Urinalysis demonstrated no abnormalities. Scrotal ultrasound showed normal bilateral testicular parenchyma with the normal arterial and venous flow. It also revealed enlargement of the left epididymis with increased blood flow and reactive hydrocele.
The patient received an initial diagnosis of possible torsed appendix testis versus sterile epididymal orchitis.
The child received a discharge with instructions to limit physical activity for five days and use ibuprofen for pain as needed. His Final urine culture revealed no growth.
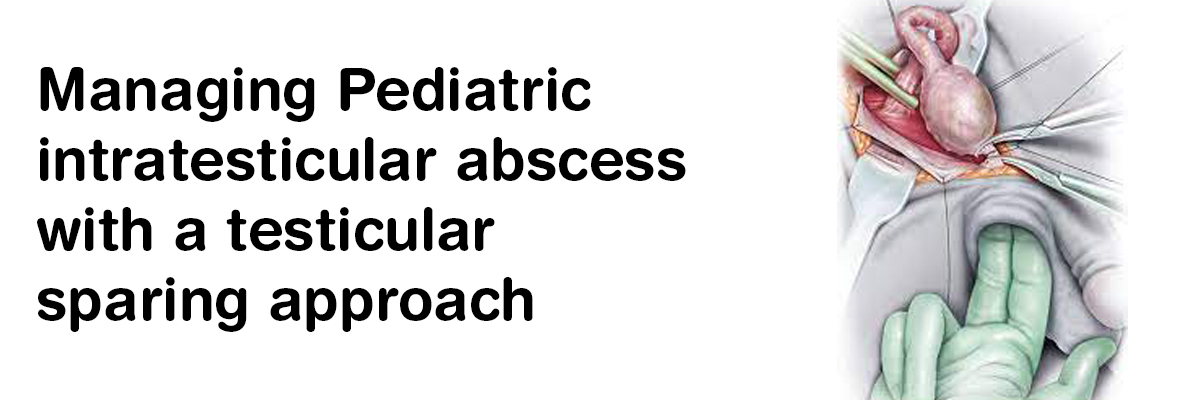
However, Eight days later, the patient returned with worsening scrotal pain and swelling. Repeat scrotal ultrasound revealed a 4cm large, complex hypoechoic collection within the left testis. He then received broad-spectrum antibiotics (ceftriaxone and vancomycin) and underwent emergency scrotal exploration. The surgeons placed a midline scrotal incision. They observed tunica vaginalis densely adherent to the tunica albuginea and the entered testicle. The surgeons immediately drained the Copious purulent material from the testicular cavity, irrigated the abscess cavity, and left it open. They placed a Jackson Pratt drain in the left hemiscrotum and performed Primary closure of the scrotal incision using 3-0 prolene retention sutures.
Postoperative renal bladder ultrasound revealed a duplicated left kidney with mild cortical thinning of the lower pole, a normal upper pole moiety, a normal right kidney, and scant debris within the urinary bladder. The surgeons removed his drain on postoperative day 3. The culture of the intratesticular abscess ultimately showed Bacteroides fragilis, Parvimonas micra, Escherichia coli, and Streptococcus anginosus. Antibiotic sensitivities prompted a 14-day course of oral Amoxicillin clavulanate for the patient.
The patient then received re-evaluation two months later and showed normal scrotal examination findings, with ultrasound revealing a scalloped, slightly smaller left testis with normal arterial and venous flow.
Lurz K, et al. Pediatric intratesticular abscess managed with a testicular sparing approach: A case report. Urology Case Reports. 2020;40. https://doi.org/10.1016/j.eucr.2021.101873.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs



Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article