 IJCP Editorial Team
IJCP Editorial Team
Managing an incarcerated uterus in a gynaecological patient surgically.
A report describes a case of a 46-year-old gravida 3, para 3-0-0-3 woman who presented with the inability to void completely for the last two days.
She was anuric at the time of presentation and reported regular menses, three previous spontaneous vaginal deliveries, and an abdominal myomectomy 14 years back. She also reported a history of high-grade squamous intraepithelial lesions, and a colposcopy had demonstrated ectocervical disease. Her recent imaging studies demonstrated multiple intramural leiomyomata and adenomyosis.
Physical examination revealed a grossly enlarged uterus measuring over 10 cm filled the posterior cul de sac. Her cervix was not palpable and wasn't visible during the speculum examination. She underwent Foley catheter placement, followed by one liter of urine drainage. An ultrasound scan demonstrated an enlarged uterus, measuring 13.4 × 0.8 × 10 cm, with multiple leiomyomas (fundal leiomyoma of 2.6 × 2 × 2.5 cm; posterior lesion of 6.5 × 3 × 5 cm, and a central leiomyoma of 8.2 × 8.1 × 8.1 cm).
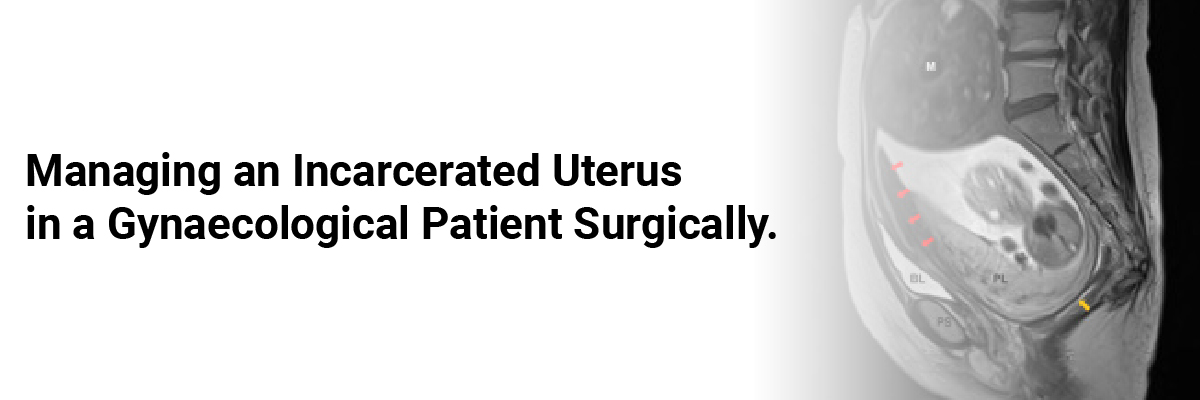
Magnetic resonance imaging (MRI) revealed an anteriorly displaced cervix and no hydronephrosis.
She was educated about all the possible treatment strategies but opted for operative reduction with an abdominal hysterectomy, as she was not concerned about childbearing but was concerned about recurrence and the possibility of sarcomatous change in the leiomyomata.
The intraoperative picture revealed an enlarged uterus with multiple leiomyomata wedged deep in the pelvis and impacted upon the sacrum. Her pelvic anatomy was markedly distorted. The anterior and lateral aspects of the uterus were clear of adhesions, with the cervix not visible or easily palpable. Her bladder and peritoneal reflection seemed stretched out, with the latter folded over on itself, possibly indicative of the early stages of uterine sacculation.
The surgeons sharply released the folded-over bladder reflection, which normalized the local anatomy. They placed a traction suture in the anterior fundus to mobilize the uterus, which failed. After considering the options, the surgeons carefully employed a Doyen tumor screw with Furniss modification. Then they slowly elevated the uterus with traction in an upward and slightly caudal direction (away from the sacral promontory). They observed a vacuum-like suction release on the release of impaction. The uterus had multiple leiomyomata of varying sizes, with two dominant posterior lesions.
The surgery remained uncomplicated, and the patient tolerated the procedure well. She urinated without difficulty on a postoperative day one and had minimal post-void residual urine.
She received a discharge in stable condition on postoperative day 3. At follow-up, she no longer had urinary complaints. Her surgical pathology was remarkable for adenomyosis, multiple myomas, and cervical intraepithelial neoplasia III.
Fahimuddin FZ, Murphy R, O'Shaughnessy M. Surgical management of an incarcerated uterus in a gynecological patient: A case report. Case Reports in Women's Health. 2019;23. https://doi.org/10.1016/j.crwh.2019.e00123.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs

Related FAQs










Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article