 IJCP Editorial Team
IJCP Editorial Team
Early diagnosis of placenta accreta in a mid-trimester post-abortal hemorrhage case
Placenta accreta, an obstetric emergency associated with life-threatening risks, can also complicate abortions in the first and second trimesters – presenting as excessive vaginal bleeding and challenges in placenta removal. A history of multiple cesarean deliveries is a significant risk factor. Given the high-risk nature, suspected instances of the placenta accreta spectrum necessitate early diagnosis and multidisciplinary team involvement to ensure better maternal and fetal outcomes.
Case report: A 36-year-old lady presented to the labor room and reported experiencing bleeding during her antenatal period.
She had previously undergone three cesarean sections (C-sections) and had a history of retained placenta with heavy vaginal bleeding,
Upon initial examination, her pulse rate was 118 per minute, blood pressure was 90/60 mm Hg, and oxygen saturation was 98% in room air. There were no signs of pallor, jaundice, cyanosis, clubbing, or pedal edema. On abdominal examination, the uterus was not well-contracted and was located below the umbilicus. Vaginal examination revealed an open os and a retained placenta, with torrential vaginal bleeding.
An initial resuscitation was performed, and oxytocic medication was administered, but placental separation did not occur, and the bleeding persisted. Due to the severe bleeding and the patient's history of three prior C-sections, she was immediately taken to the operating room for an exploratory laparotomy with a provisional diagnosis of a morbidly adherent placenta and severe hemorrhage.
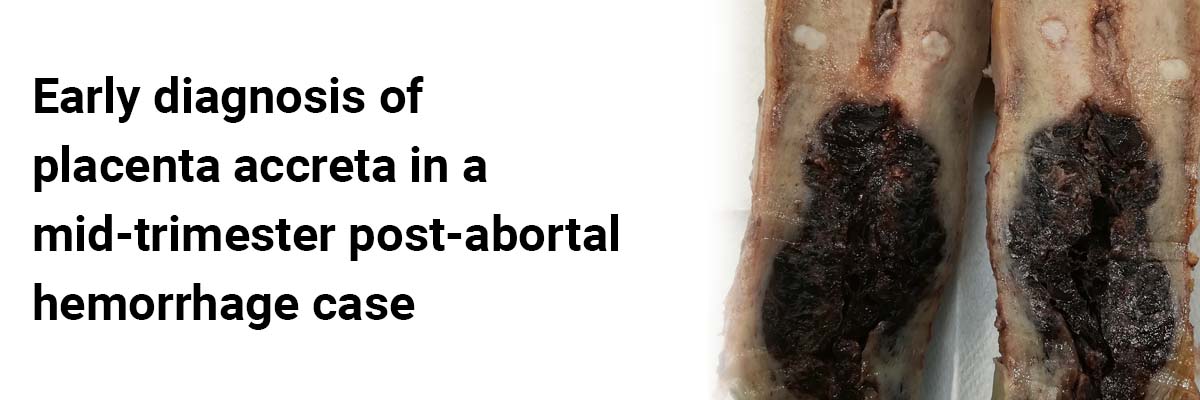
During the surgery, it was observed that the anterior surface of the lower uterine segment was entirely covered by engorged blood vessels, while the bladder was unaffected. A subtotal hysterectomy was performed, achieving hemostasis to address the morbidly adherent placenta. Two units of packed red blood cells were transfused during the surgery, and the patient was subsequently moved to the ICU for postoperative monitoring. She recovered well and was discharged on postoperative day six.
The histopathological examination of an enlarged uterus specimen (9x8x6cm) with an adherent placenta in the lower segment, taken from the upper segment of the uterus, revealed findings consistent with pregnancy-related changes in the uterus with placenta accreta. These findings included a secretory endometrium with decidualization, a few trophoblastic cells in the endometrial lining, and myometrial hypertrophy with congested blood vessels and edema. The section from the adherent placenta showed chorionic villi attached to the myometrium without invasion.
Post-abortal hemorrhage can be critical and should be deemed an emergency associated with maternal mortality and morbidity. While a hysterectomy is the standard procedure for the placenta accreta spectrum, early identification, prompt decision-making, and timely intervention can be life-saving.
Source: Gautam A, Malik N, Jain S. Indian J Obstet Gynecol Res. 2023;10(3):362-365
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs

Related FAQs










Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article