Primary Gout in a 6-Year-Old Girl Presenting as a Foot Mass: A Case Report
A report describes a case of a 6-year-old girl who presented with swelling on the lateral dorsum and little toe of her right foot, initially measuring approximately 0.5 cm in diameter in April 2023, and diagnosed as a "vascular malformation" at a local hospital. Despite topical sirolimus treatment, the lesion gradually enlarged to 1.5 cm by August 2023. At this point, a second opinion suggested a "thick fluid cyst." The family opted for conservative follow-up. Over time, the swelling increased to 2.5 cm, and the patient was diagnosed with a "sebaceous cyst" in November 2023 and was given oral antibacterial drugs and hot compresses. By January 2024, it reached 4 cm, causing pain and difficulty wearing shoes, prompting hospital admission.
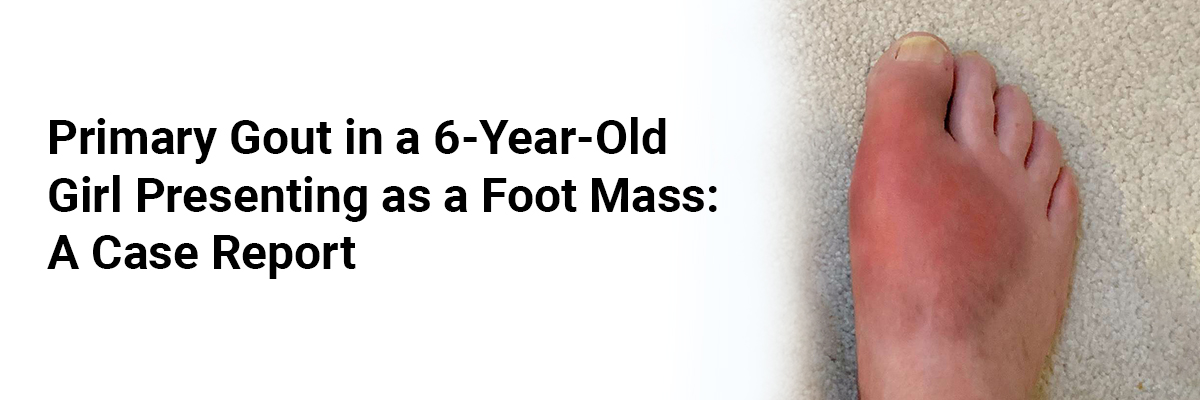
On admission, the patient's blood pressure was 108/66 mmHg (90th percentile), weight 29 kg (97th percentile), height 130 cm (75th percentile), and body mass index (BMI) 17.2 kg/m² (90th percentile). Examination revealed a 4-cm oval, soft, broad-based swelling with slight redness over the lateral dorsum of the right foot, without tenderness, open wounds, bleeding, or bony friction. Systemic examination was unremarkable.
Patient's father had a history of gout, and the patient revealed a history of regular consumption of high-fructose beverages for the past 2 years. Laboratory testing showed elevated serum uric acid at 6.25 mg/dL, while other parameters, including renal and hepatic function, blood counts, inflammatory markers, autoantibodies, immunoglobulins, and lymphocyte subsets, were within normal limits. Urinary tract ultrasonography was routine.
An ultrasound of the foot revealed a subcutaneous mass over the fifth toe and the lateral foot. Radiographs showed a dense nodular mass around the fifth metatarsal and phalanges. Magnetic resonance imaging (MRI) revealed abnormal subcutaneous soft tissue signal between the fourth and fifth toes and the right foot's lateral aspect of the fifth metatarsal. Enhanced computed tomography (CT) confirmed dense soft tissue shadows in the same region. Based on the patient's history and the clinical, laboratory, and imaging findings, a diagnosis of primary gout with hyperuricemia was made.
Surgical excision of the mass was done. Postoperatively, serum uric acid increased to 9.6 mg/dL. Histopathology showed extensive urate crystal deposits and multinucleated giant cell reaction within fibrous tissue, confirming gout. Genetic testing via next-generation sequencing identified variants in ABCG2 (c.421C>A), SLC2A9 (c.881G>A), SLC22A12 (c.831-192C>A), and MTHFR (c.677C>T). Metabolic investigations, including urinary organic acids, amino acids, and acylcarnitine profiles, were normal.
The patient was started on a low-purine diet, oral febuxostat 10 mg/day, sodium bicarbonate 0.25 g three times daily, and increased hydration. Follow-up showed gradual normalization of serum uric acid to 4.48 mg/dL, good wound healing, and absence of pain or recurrence. The patient has been under regular outpatient follow-up for 1 year.


Recent FAQs





Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article