 IJCP Editorial Team
IJCP Editorial Team
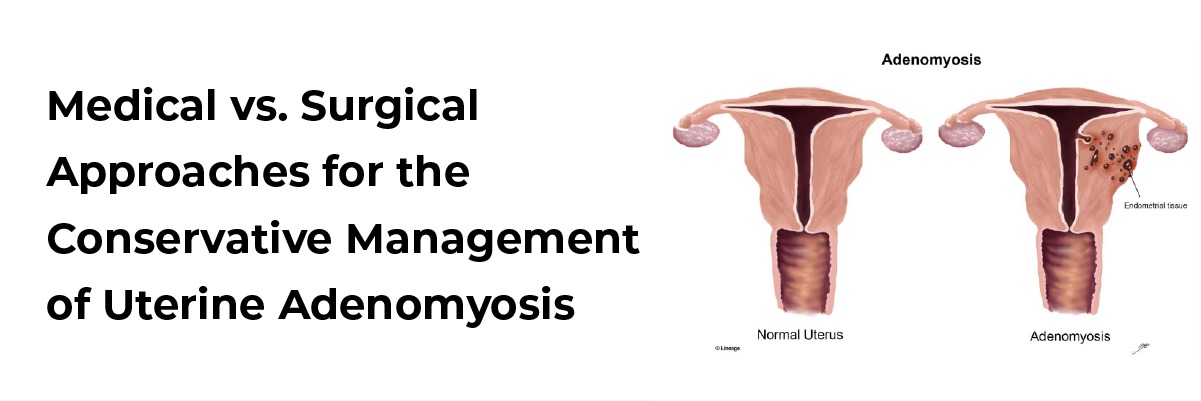
Medical vs. Surgical Approaches for the Conservative Management of Uterine Adenomyosis
Uterine adenomyosis is a commonly encountered estrogen-dependent disease in reproductive-age women, causing heavy menstrual bleeding, intense pelvic pain, and infertility. Uterine adenomyosis affects approximately 20% of gynecology patients. Although adenomyosis was previously considered a disease of multiparous women, it has become increasingly evident that it also affects younger nulliparous women compromising their fertility potential. Thus, a lack of critical information on the origin of the disease and the absence of a universal classification system created a kind of therapeutic anarchy leading to 82% of adenomyosis patients resorting to hysterectomy, a somewhat extreme way to deal with the disease. It is clear that hysterectomy, the standard approach to managing the disease, is not an option for patients wishing to preserve their fertility.
On the other hand, there is no existing drug that can cure adenomyosis at present, but some off-label treatment options may be used to tackle disease symptoms and improve fertility outcomes. Currently, medical therapies for adenomyosis are aimed at alleviating local hypoestrogenism and tackling the most severe symptoms of adenomyosis, such as heavy menstrual bleeding, dysmenorrhea, and non-menstrual pelvic pain. Non-steroidal anti-inflammatory drugs (NSAIDs) are the most frequently prescribed class of drugs to treat dysmenorrhea, especially primary dysmenorrhea, showing acceptable efficiency but being prone to adverse side effects when used extensively. Also, combined oral contraceptives (COCs) are used to inhibit follicle-stimulating hormone (FSH) and luteinizing hormone (LH). Inhibition of FSH and LH subsequently blocks follicle development and endometrial proliferation, thereby treating adenomyosis-related symptoms.
Another alternative medical therapy for uterine adenomyosis is Gonadotropin-Releasing Hormone (GnRH) Agonists. GnRH agonist competitively binds to the natural GnRH receptors but has a longer life span than the endogenous peptide. These agonists have been used on the basis that adenomyosis relies on its anti-proliferative effects in the myometrium, following the suppression of gonadotropin secretion and the subsequent drastic decline in estradiol. Despite these promising results, GnRH agonists are associated with severe hypoestrogenic side effects, especially a reduction in bone mineral density. Hence, they cannot be used for the long-term, while on the other hand symptoms tend to reappear upon treatment cessation.
The first conservative surgical therapy for adenomyosis in young women, namely adenomyomectomy, dates back to 1952. Surgical approaches are classified into conservative partial or complete adenomyosis excision. Wedge resection or conservative partial excision involves identifying the seromuscular layer where the adenomyoma is located, before removing parts of the affected serosa and uterine adenomyosis. In complete excision, the triple flap method is performed to remove adenomyosis and reconstruct the uterine wall with a view to future pregnancy. Similarly, the asymmetric dissection method is an alternative approach that involves incision of the uterus longitudinally and dissection of the myometrium diagonally, before making a transverse incision to open the uterine cavity. But uterine rupture was observed in 5 cases out of a series of 1349 patients undergoing this technique.
Reference: Stratopoulou CA et al., J Clin Med. 2021 Oct 22;10(21):4878.
IJCP Editorial Team
Comprising seasoned professionals and experts from the medical field, the IJCP editorial team is dedicated to delivering timely and accurate content and thriving to provide attention-grabbing information for the readers. What sets them apart are their diverse expertise, spanning academia, research, and clinical practice, and their dedication to upholding the highest standards of quality and integrity. With a wealth of experience and a commitment to excellence, the IJCP editorial team strives to provide valuable perspectives, the latest trends, and in-depth analyses across various medical domains, all in a way that keeps you interested and engaged.
More FAQs by IJCP Editorial Team









Recent FAQs

Related FAQs










Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article