Managing Dermatoses of Pregnancy: Focus on ICP and PPP
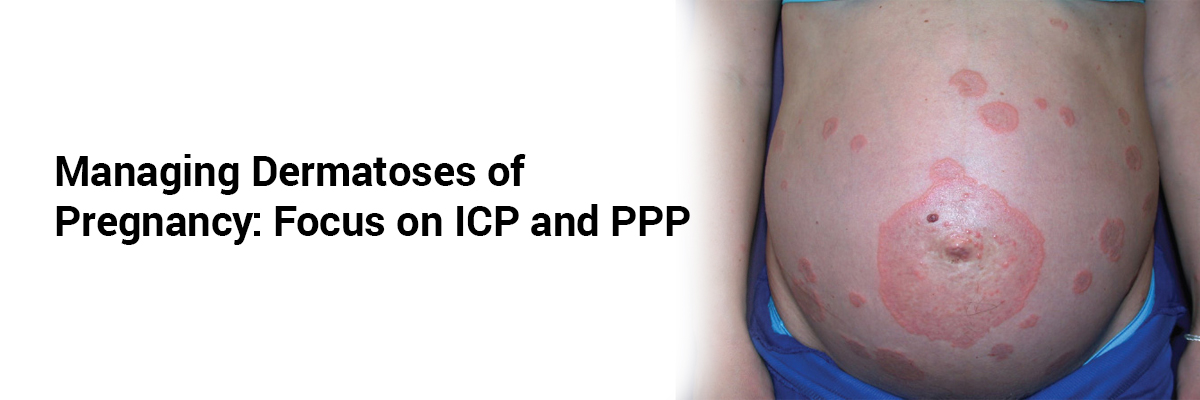
Pregnancy induces diverse cutaneous changes, ranging from benign physiological shifts to more serious dermatoses that demand clinical attention. Among these, Intrahepatic Cholestasis of Pregnancy (ICP) and Pustular Psoriasis of Pregnancy (PPP) stand out due to their systemic involvement and potential fetal risk. ICP, typically emerging in the third trimester, presents with intense pruritus and elevated serum bile acids, which may lead to adverse outcomes such as preterm birth and stillbirth. Management centers on ursodeoxycholic acid (UDCA) at 10–15 mg/kg/day (up to 21 mg/kg), which alleviates maternal symptoms by reducing bile acid levels in maternal and fetal compartments. Other supportive therapies include antihistamines, S-adenosylmethionine, and rifampin, though delivery is often recommended at 36–37 weeks, depending on bile acid levels and fetal well-being. In contrast, PPP, a rare but potentially life-threatening dermatosis occurring in late pregnancy, manifests as pustular plaques with systemic symptoms such as fever and nausea. Treatment typically involves oral corticosteroids (prednisolone 15–30 mg/day, titrated up to 60–80 mg if needed), supplemented with topical steroids and, in refractory cases, immunosuppressants such as cyclosporine or TNF inhibitors. Prompt diagnosis and individualized treatment plans are critical to improving maternal outcomes while minimizing fetal risks. Clinicians should remain vigilant, as both conditions may recur in future pregnancies or postpartum, underscoring the importance of preconception counselling and multidisciplinary care.
Source: Dermatoses during Pregnancy. Vol. March–April, Journal of South Asian Federation of Obstetrics and Gynaecology. 2025 May p. 259–63. Available from: https://creativecommons.org/licenses/by-nc/4.0/


Recent FAQs





Related FAQs










Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article