A Case of Meningococcal Pericarditis Uncommon Complication of Purpura Fulminans
1. Purulent
pericarditis – due to direct bacterial invasion
2. Immunologic
pericarditis – due to immune-mediated inflammation
3. Chronic
constrictive pericarditis – a late sequela
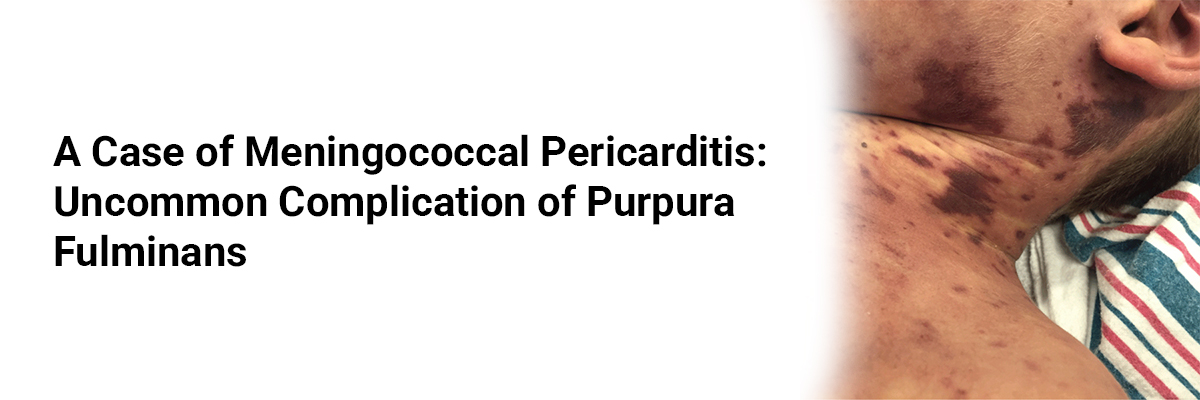
Although Neisseria meningitidis commonly presents with meningitis
or septicemia, cardiac involvement is rare. Purpura fulminans, characterized by
rapidly progressive cutaneous hemorrhagic necrosis, indicates severe sepsis and
carries a high mortality risk.
On examination:
·
BP: 80/50 mmHg, HR: 120 bpm
·
Extensive purpura over lower limbs and trunk
·
Muffled heart sounds and distended neck veins
·
Signs of septic shock
Investigations:
·
CBC: Leukocytosis with neutrophilia
·
Coagulation profile: Prolonged PT and aPTT, low
fibrinogen
·
Blood cultures: Neisseria meningitidis
serogroup C
·
Echocardiography: Large pericardial effusion
with early tamponade features
·
Skin biopsy: Dermal vessel thrombosis with
fibrin deposition (consistent with purpura fulminans)


Recent FAQs





Related FAQs









Medtalks is India's fastest growing Healthcare Learning and Patient Education Platform designed and developed to help doctors and other medical professionals to cater educational and training needs and to discover, discuss and learn the latest and best practices across 100+ medical specialties. Also find India Healthcare Latest Health News & Updates on the India Healthcare at Medtalks
Please login to comment on this article